On June 23 local time, the international authoritative immunology journal Science · immunology published the heavy research: the antigen map showed that compared with the original Xinguan strain and the previous variant strain, Omicron ba 1 and ba The antigen evolution of 2 shows two “outliers”, and there is also a large distance between the two “outliers”. Meanwhile, ba 1 and ba Because of their different antigenic characteristics, they escaped the antibody response induced by the vaccine (mRNA vaccine, bnt162b2)< img alt="" style="width:600px;" src=" https://imagecloud.thepaper.cn/thepaper/image/202/382/394.jpg "> the aforementioned research teams include the medical school of Erasmus University in Rotterdam, the Netherlands, and the University of Cambridge in the United Kingdom. The medical school of Erasmus University in Rotterdam, the Netherlands, together with the Karolinska medical school in Sweden and the medical school of the University of Leuven in Belgium, are known as the” three major medical schools in Europe “.
antigen It refers to the substance that can induce the immune response of the body, that is, the substance that can be specifically recognized and combined by the antigen receptor (tcr/bcr) on the surface of t/b lymphocytes, activate t/b cells, make them proliferate and differentiate, produce immune response products (sensitized lymphocytes or antibodies), and can specifically bind with corresponding products in vivo and in vitro< Br>
antigenic substances have two important characteristics: immunogenicity and immunereactivity. Immunogenicity refers to the ability of antigens to induce specific immune responses and produce antibodies and / or sensitized lymphocytes; Immunoreactivity refers to the ability to react specifically with corresponding immune effectors (antibodies or sensitized lymphocytes) in vitro and in vivo< Br>
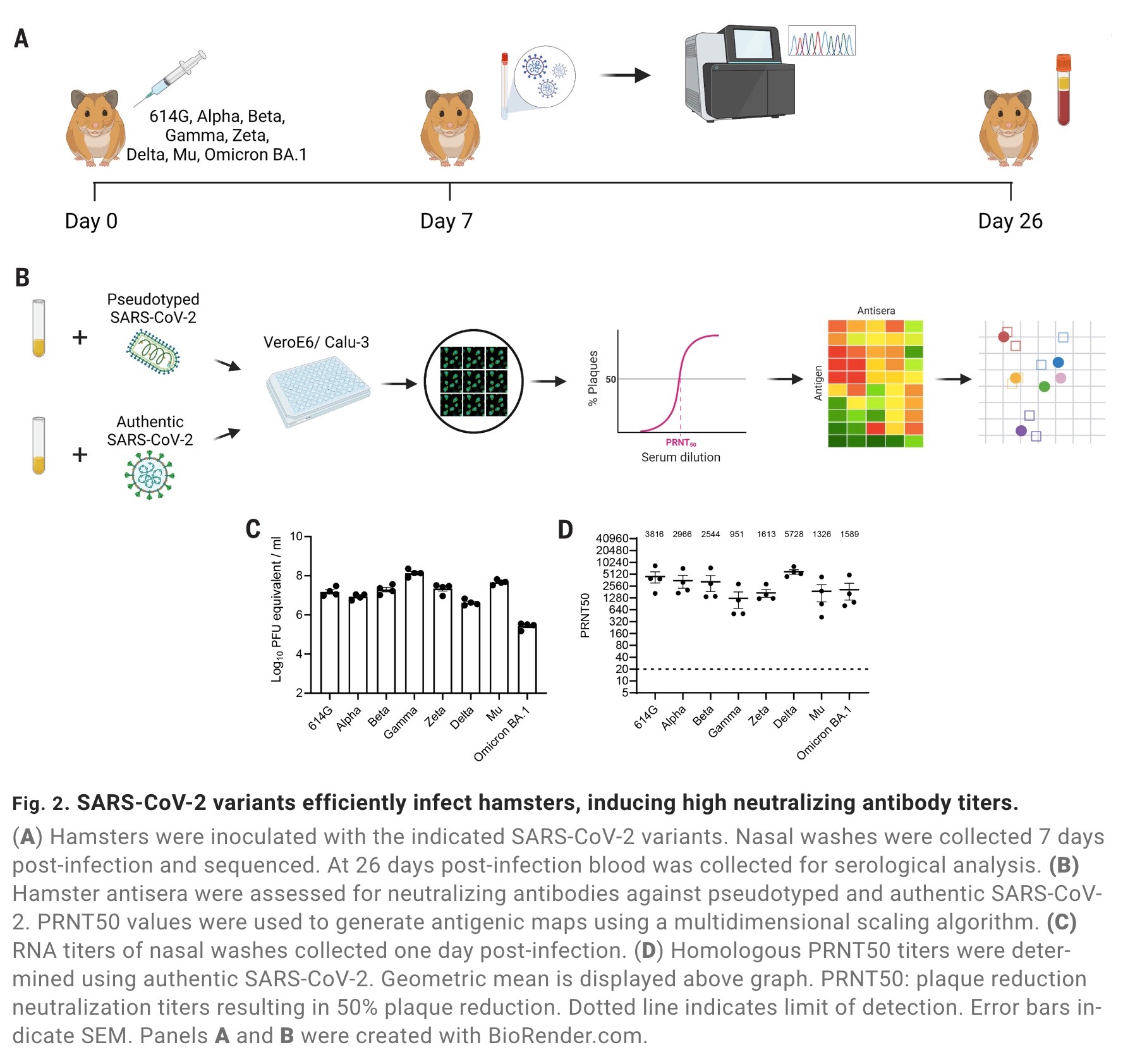
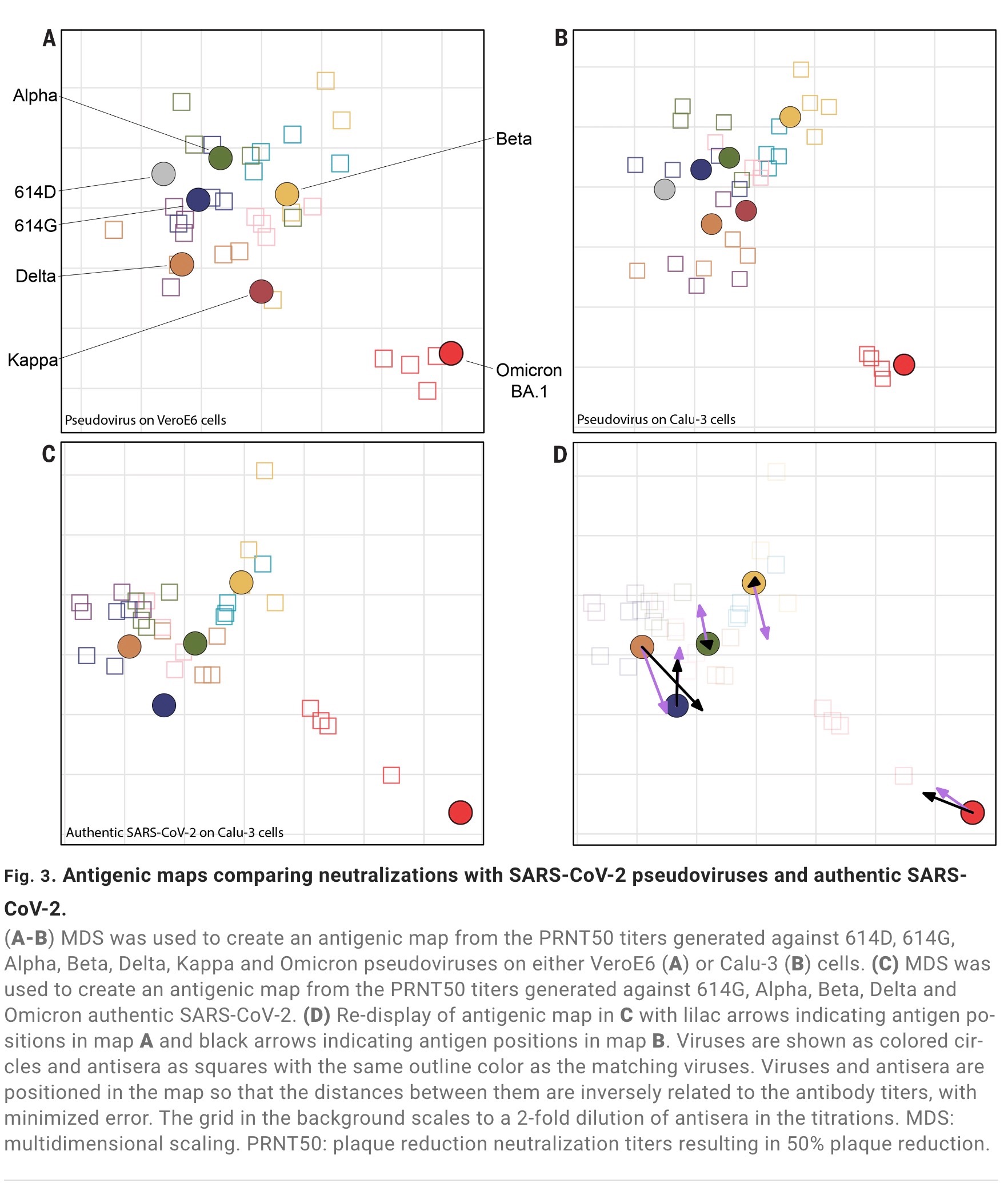
the previous studies used antigen maps to visualize early new crown variants (614g α、 Beta、 γ、 Zeta, Delta and mu) and quantify this difference. The researchers used hamster serum obtained after primary infection. They first verified that the selection of cell lines for neutralization assay had no substantial effect on the topology of the map. The results of the antigenic map generated by pseudotyped sars-cov-2 on the widely used veroe6 cell line and the antigenic map generated by human airway cell line Calu-3 are similar< Br>
the map produced by using real sars-cov-2 on Calu-3 cells is also very similar to the map generated by false typing. The antigenic map revealed that the early variant strains of sars-cov-2 showed a central cluster. These early variant strains of novel coronavirus are similar in antigen and relatively close to each other in antigen space< Br>
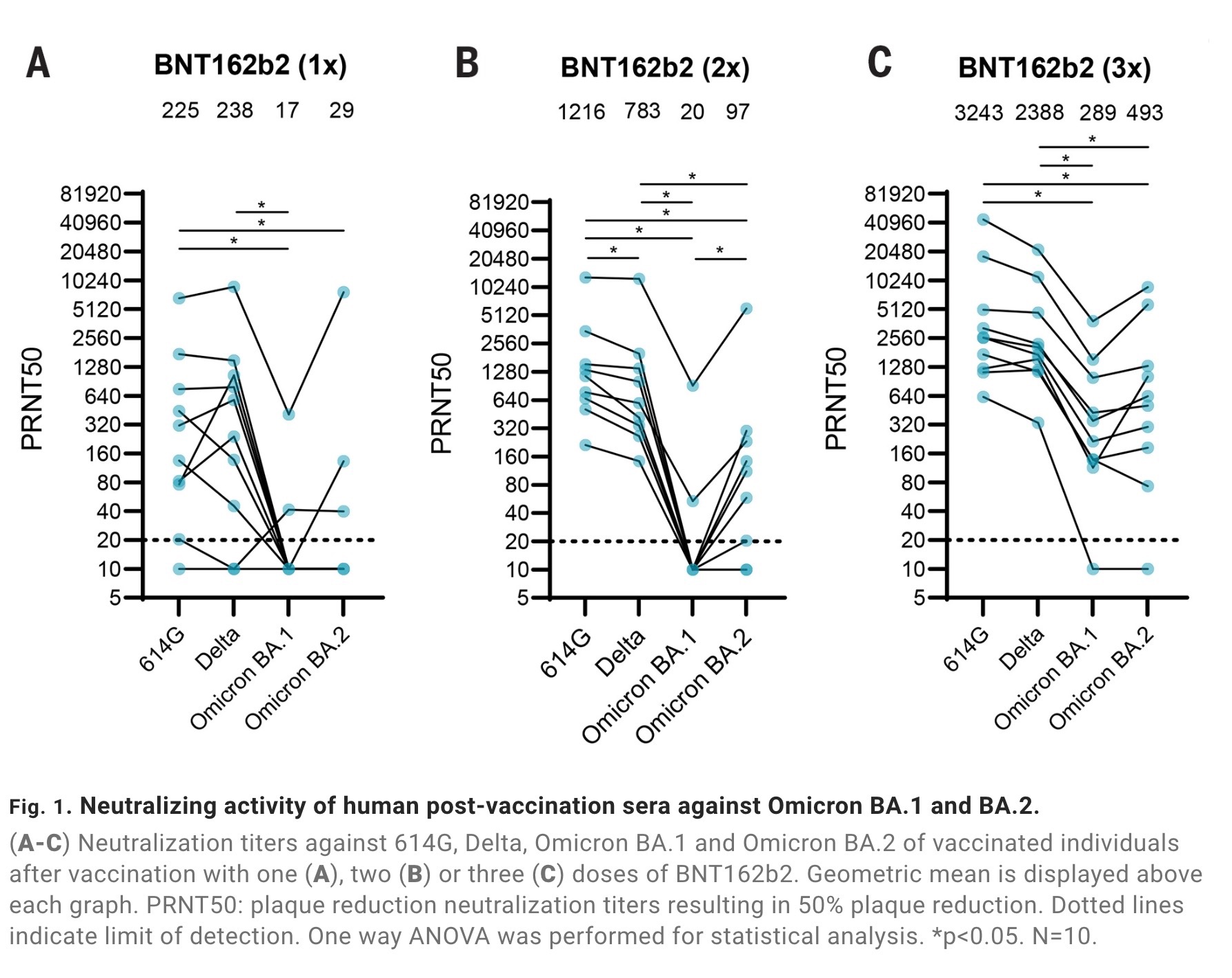
however, the study found that Omicron ba 1 and ba 2 has evolved into two different antigenic outliers. Research data show that ba 1 and ba Because of their different antigenic characteristics, they escaped the antibody response induced by the previous vaccine. Therefore, the antigenic map can be used to evaluate the antigenic characteristics of the worrying sars-cov-2 variant in the future and determine the composition of a new spike protein based (enhanced) vaccine< Br>
the influenza virus has been circulating in the human world for hundreds of years. By comparison, the epidemic time of novel coronavirus (sars-cov-2) in human society is still short, less than 3 years. Before the emergence of the Omicron variant of novel coronavirus, most novel coronavirus variants contained only a few mutations in the spike protein, the “key” to human cells, and were still recognized by human sera during the recovery period of infection and after vaccination< Br>
however, the rapid emergence of new variants of novel coronavirus may have a significant impact on the efficacy of the vaccine. Omicron ba 2 gene sequence and Omicron original strain ba 1 it is very different, and it completely replaces BA in the world 1, but ba The antigenic properties of 2 have not been evaluated, and this study answers this question< Br>
this study also answers why a large number of overseas people are infected with Omicron ba After 1, Ba will still be repeatedly infected 2。 At the same time, ba 1、BA. After 2, ba 2.12.1、BA. 4/5 can still cause a large number of repeated infections, and significant differences in antigens are also the key factors< Br>
on June 22, the international authoritative academic journal New England Journal of Medicine (NEJM) published the latest research from Beth Israel Deaconess Medical Center of Harvard University. It was found that the neutralizing antibody titer of subjects was significantly lower than that of ba 4/5 was 21 times lower than the original strain of novel coronavirus. At the same time, this study also shows that ba 2.12.1 、BA. 4 and ba 5 can also escape infection with ba 1、BA. 2 brings about immunity. This study is ba 2.12.1 、BA. 4 and ba Why it can cause breakthrough infection (still infected after vaccination) and repeated infection provide support< Br>
different antigens and multiple repeated infections pose a major challenge to health. Previous studies have shown that the first infection with novel coronavirus (sars-cov-2) will increase the risk of disease, death and sequelae. However, whether reinfection of new crowns will further increase the risk has not been systematically studied. With at least 500million people worldwide infected with the new crown, the Omicron variant ba 4/5 has stronger immune escape ability and reinfection ability, so it is urgent to study reinfection. Recently, the Washington University School of medicine and the St. Louis veterans health care system jointly released the “outcomes of sars-cov-2 infection”< Br>
the previous study found that compared with the first time infected with the new crown, reinfected people showed an increase in all-cause mortality, hospitalization and many disease risks through the analysis of a large sample of 5.69 million people. The risk is significantly increased for people who have not been vaccinated or who have received one or two or more injections before the second infection< Br>
the risk of repeated infection is most obvious in the acute phase, but it still exists after the acute phase of reinfection. The risk of most sequelae is still obvious at 6 months. Compared with the uninfected control group, the assessment of the cumulative risk of repeated infection showed that the risk of all-cause death, excess burden and other diseases increased sharply with the increase of the number of infections. That is to say, the risk is the lowest among those infected for one time, increased among those infected for two times, and the highest among those infected for three or more times< Br>
attached: important charts