Editor’s note: Why do patients develop different outcomes after being infected with new coronavirus? Which part of the patient may change from mild and common to severe or worse? This is not only a matter of public concern, but also has important guiding significance for the subsequent prevention and control of the epidemic.
Hou Jinlin, director of the Liver Disease Center of the Southern Hospital of Southern Medical University and director of the Guangdong Liver Disease Research Institute, just returned to work from the front line of aid to Hubei, April 16 In the sixth issue of “Understanding the Future” Scientific Lecture: Viruses and Human Health-Special Science Popularization, he launched the “Honghu Model” of managing the infection of the new coronavirus in the sixth issue of “Understanding the Future” Scientific Lectures organized by the Future Forum of Scientific Nonprofit Organizations
Hou Jinlin introduced that in the field of infectious diseases, some bacteria and viruses will have an “iceberg phenomenon” after infection, because a small number of patients will cause serious infections and death. Most patients are light or normal. A certain percentage of patients are hidden infections or subclinical infections. There are also some people who have not been infected after exposure. The classification of patients depends on the body’s immunity, which is the result of the interaction between the virus and the body’s immunity.
The research team structurally analyzed light and moderate patients in 33 hospitals in Guangdong Province, a total of 1138 patients. We used 818 patients as the modeling team, and 320 mild patients screened by Wuhan Hankou Hospital and Honghu Hospital of Hubei Province as the verification group. It can be clearly seen that there is no difference between men and women. After multi-factor analysis, the indicators of age, history of chronic disease, ratio of white blood cells and lymphocytes, whether C-reactive protein is greater than 25 and D-dimer are screened. The patients were divided into low-risk group, medium-risk group and high-risk group accordingly. Almost 40% of the patients in the high-risk group will change into aggravation within 14 days of hospitalization.
Hou Jinlin hopes to use this critical risk early warning model to analyze which indicators may cause the patient to worsen. Especially in high-endemic areas, if the possibility of exacerbation of patients can be detected as soon as possible, and then focus on management and intervention, it is possible to avoid serious consequences.
The full text of the speech was organized by Guo Lijie, a PhD student at the Institute of Biophysics, Chinese Academy of Sciences. Surging news is sorted and released twice after being authorized.
Hou Jinlin: Talking about the asymptomatic infection of New Coronavirus from the clinical characteristics and outcome of viral infection
Hou Jinlin: Talking about the asymptomatic infection of New Coronavirus from the clinical characteristics and outcome of viral infection
Thank you very much for the future forum to invite me to share with you My experience about new crown infection. I am a staff member of the Department of Infectious Medicine of Southern Hospital. About 80% of my usual work is mainly in the treatment of liver diseases, and the other 20% is dealing with other infectious diseases. This time I was temporarily transferred to Jingzhou, Hubei for prevention and control of the new crown. Tonight, I want to share with you some of my own knowledge, including the analysis of the indicators for the increase of early warning of new coronary pneumonia, asymptomatic infection data, etc. These data have not been published so far, so please criticize and correct.
First, let me report to you on our situation in Honghu. Asymptomatic infections have recently attracted everyone’s attention as a hot spot. Let’s take a look at the characteristics of general viral infections to further understand asymptomatic infections. In fact, the new coronavirus can cause a variety of disease spectrum, and there are some clinical early warning indicators that can predict whether these patients will become more severe or critically ill. When he was in Honghu, Secretary of the Party Committee of Nanfang Hospital personally led the team, hoping to establish a Honghu model for managing the infection of the new crown virus in Honghu. This model not only focuses on the treatment of hospital patients, but also on community screening.
I arrived in Jingzhou, Hubei on January 10 and returned to Guangzhou on March 20. During this period, I have visited places such as Jinghu Honghu and Wuhan Hankou to help discuss in these places To coordinate the work of the two medical teams of our hospital in Hankou and Honghu.
Honghu is a land of fish and rice. Honghu City has a population of 950,000, which is about 1.5-2 hours ’drive from Wuhan. After we went to Honghu, we liked this place very much. Even many of our colleagues in the medical team of Southern Hospital said they were willing to work hard for Honghu. The government leads and unifies the planning, integrates the entire Honghu medical unit, classifies the treatment by functions, and then performs comprehensive treatment. Here we have designed an early warning area based on the severity of the condition, and at the same time, the recovered patients will remain in the rehabilitation area for follow-up and management.
When we went, we brought 4 laboratory staff to detect antibodies in 8000 patients using two antibody kits (colloidal gold and chemiluminescence method) . In addition, we have established a big data platform in cooperation with China Medical. In the next stage, we will make plans to go to Honghu to carry out hepatitis elimination.
Just said that Honghu to Wuhan is a 1.5-hour drive with a population of 950,000, of which 100,000 are in Wuhan, and 55,000 people returned to Honghu before the closure of Wuhan 45,000 people were trapped in Wuhan, with more than 1,100 hospitalizations related to Xinguan, 363 nucleic acid diagnoses, 15 deaths, 1/4 of critically ill patients, and more than 320 suspected patients. In addition, there are more than 300 community-level segregated people in various townships, including asymptomatic peopleMore than 50 people. When we left, Honghu had no new confirmed cases for 20 consecutive days. When we were in Honghu, we almost met with Mayor Shen Xianwu of Honghu every day to discuss and arrange epidemic prevention and control. He also signed on my clothes. I think the local people in Honghu are very affectionate and meaningful.
We signed a long-term cooperation agreement with them, hoping to further carry out the work on eliminating viral hepatitis in Honghu, and hope that there will be a follow-up project on hepatitis B mother-to-child transmission .
01 virus infection characteristics overview
01 virus infection characteristics overview
For the asymptomatic infections that people are particularly concerned about recently, different professional understandings are different, and even caused controversy. Here we explain to the general public how to understand the characteristics of the disease after infection, the characteristics, mechanism and significance of asymptomatic infection.  In fact, there are many types of diseases caused by viral infections, New Coronary Pneumonia is a disease transmitted by the respiratory tract. Hepatitis B can be transmitted by mother and child, and AIDS can be transmitted by blood. Here we specifically mention that the infection of the new coronavirus is mainly transmitted through the respiratory tract, and there is the possibility of aerosol transmission in a relatively closed environment. There were previous reports that the nucleic acid of the new coronavirus was detected in feces, but it is unclear whether it will affect the entire epidemic prevention and control. There will be vertical transmission of hepatitis B and HIV infection, but the new coronavirus has not found evidence of vertical transmission.
In fact, there are many types of diseases caused by viral infections, New Coronary Pneumonia is a disease transmitted by the respiratory tract. Hepatitis B can be transmitted by mother and child, and AIDS can be transmitted by blood. Here we specifically mention that the infection of the new coronavirus is mainly transmitted through the respiratory tract, and there is the possibility of aerosol transmission in a relatively closed environment. There were previous reports that the nucleic acid of the new coronavirus was detected in feces, but it is unclear whether it will affect the entire epidemic prevention and control. There will be vertical transmission of hepatitis B and HIV infection, but the new coronavirus has not found evidence of vertical transmission. 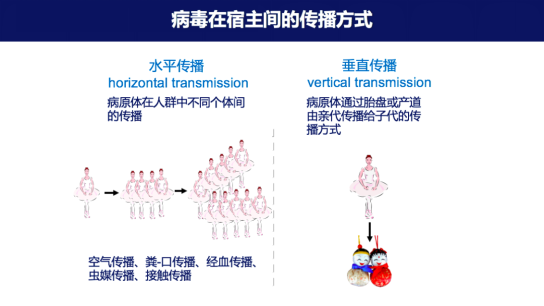 The source of infection of the new crown virus except for symptomatic patients It also involves people with asymptomatic infections. Everyone is concerned about the proportion of asymptomatic infections, because different studies or models derive different denominators, so the proportion of reported asymptomatic infections varies greatly. Low 1% -2%, high 40% -60%.
The source of infection of the new crown virus except for symptomatic patients It also involves people with asymptomatic infections. Everyone is concerned about the proportion of asymptomatic infections, because different studies or models derive different denominators, so the proportion of reported asymptomatic infections varies greatly. Low 1% -2%, high 40% -60%.  It is generally believed that the virus can be localized in the host body after infection Spread, local spread refers to the virus invading the body and proliferating in local tissues, such as enteroviruses in the pharyngeal epithelial cells and localLymphoid tissues, respiratory viruses multiply in the epithelial cells of the upper respiratory tract mucosa to form infections. But most classic viruses spread through the body, infect through the blood and lymphatic system, and then form two viremias. Therefore, after the virus infection, there can be local infection, only invading local cells, and it can also form a systemic infection. After the blood, lymph and nerve tissue spread, it causes damage to multiple organs and systems.
It is generally believed that the virus can be localized in the host body after infection Spread, local spread refers to the virus invading the body and proliferating in local tissues, such as enteroviruses in the pharyngeal epithelial cells and localLymphoid tissues, respiratory viruses multiply in the epithelial cells of the upper respiratory tract mucosa to form infections. But most classic viruses spread through the body, infect through the blood and lymphatic system, and then form two viremias. Therefore, after the virus infection, there can be local infection, only invading local cells, and it can also form a systemic infection. After the blood, lymph and nerve tissue spread, it causes damage to multiple organs and systems.
In fact, there are many types of diseases caused by viral infections, New Coronary Pneumonia is a disease transmitted by the respiratory tract. Hepatitis B can be transmitted by mother and child, and AIDS can be transmitted by blood. Here we specifically mention that the infection of the new coronavirus is mainly transmitted through the respiratory tract, and there is the possibility of aerosol transmission in a relatively closed environment. There were previous reports that the nucleic acid of the new coronavirus was detected in feces, but it is unclear whether it will affect the entire epidemic prevention and control. There will be vertical transmission of hepatitis B and HIV infection, but the new coronavirus has not found evidence of vertical transmission. The source of infection of the new crown virus except for symptomatic patients It also involves people with asymptomatic infections. Everyone is concerned about the proportion of asymptomatic infections, because different studies or models derive different denominators, so the proportion of reported asymptomatic infections varies greatly. Low 1% -2%, high 40% -60%. It is generally believed that the virus can be localized in the host body after infection Spread, local spread refers to the virus invading the body and proliferating in local tissues, such as enteroviruses in the pharyngeal epithelial cells and localLymphoid tissues, respiratory viruses multiply in the epithelial cells of the upper respiratory tract mucosa to form infections. But most classic viruses spread through the body, infect through the blood and lymphatic system, and then form two viremias. Therefore, after the virus infection, there can be local infection, only invading local cells, and it can also form a systemic infection. After the blood, lymph and nerve tissue spread, it causes damage to multiple organs and systems.
The result of virus infection: the interaction between the virus and the host ’s immune system maintains a dynamic balance. If the immune system is dominant and the virus is cleared, it is possible to gain immunity or not; If the virus predominates, there is a persistent infection; the mutual advantage of the two can lead to chronic infection and relapse. Obviously so far we believe that the new coronavirus is an acute infection, because the body’s immunity is dominant, and then the virus will be cleared soon, so the body’s immunity plays a very important role in controlling and removing the virus.  In the field of infectious diseases, whether it is a virus or There are different outcomes for bacterial infections. After some bacterial and viral infections, we call it the “iceberg phenomenon” because a small number of patients can cause serious infections and death, and most patients are light or ordinary. A certain percentage of patients are hidden infections or subclinical infections, and here we do not use the term asymptomatic infection. There are also some people who have not been infected after exposure. The classification of patients depends mainly on the body’s immunity, which is the result of the interaction between the virus and the body’s immunity. If the virus invades the body in a large number and replicates abnormally, it can cause severe or critical illness. After the virus invades the body, a large amount of replication produces a strong immune response, which can cause ordinary and mild infections. Viruses invading the body can produce an immune response but no obvious pathological damage. It is a recessive infection or a subclinical infection. If the virus is cleared quickly after invading the body and there is no immune response, these are not infected after exposure.
In the field of infectious diseases, whether it is a virus or There are different outcomes for bacterial infections. After some bacterial and viral infections, we call it the “iceberg phenomenon” because a small number of patients can cause serious infections and death, and most patients are light or ordinary. A certain percentage of patients are hidden infections or subclinical infections, and here we do not use the term asymptomatic infection. There are also some people who have not been infected after exposure. The classification of patients depends mainly on the body’s immunity, which is the result of the interaction between the virus and the body’s immunity. If the virus invades the body in a large number and replicates abnormally, it can cause severe or critical illness. After the virus invades the body, a large amount of replication produces a strong immune response, which can cause ordinary and mild infections. Viruses invading the body can produce an immune response but no obvious pathological damage. It is a recessive infection or a subclinical infection. If the virus is cleared quickly after invading the body and there is no immune response, these are not infected after exposure.
In the field of infectious diseases, whether it is a virus or There are different outcomes for bacterial infections. After some bacterial and viral infections, we call it the “iceberg phenomenon” because a small number of patients can cause serious infections and death, and most patients are light or ordinary. A certain percentage of patients are hidden infections or subclinical infections, and here we do not use the term asymptomatic infection. There are also some people who have not been infected after exposure. The classification of patients depends mainly on the body’s immunity, which is the result of the interaction between the virus and the body’s immunity. If the virus invades the body in a large number and replicates abnormally, it can cause severe or critical illness. After the virus invades the body, a large amount of replication produces a strong immune response, which can cause ordinary and mild infections. Viruses invading the body can produce an immune response but no obvious pathological damage. It is a recessive infection or a subclinical infection. If the virus is cleared quickly after invading the body and there is no immune response, these are not infected after exposure.
Taking epidemic meningitis as an example, only 1% -2% of people who actually develop meningitis form meningitis, and less than 10% are 90% of upper respiratory tract infections are recessive infections. There are also many other viral infections including recessive infections. For example, common hepatitis B also has recessive infections. Taking our current knowledge of the new coronavirus as an example, we still don’t know what percentage of the infection is recessive or subclinical. After taking such strict measures after the closure of Wuhan, China, large-scale antibody screening is still required for the proportion of recessive infections.
Viral infection can be acuteInfection and persistent infection.
Continuous infections include chronic infections, latent infections and lentivirus infections.
Chronic infection means that the virus can continue to exist in the body and be discharged to the body frequently or intermittently, showing asymptomatic, this long-term carrying of the virus will eventually lead to important targets Organ damage, such as the continuous accumulation of hepatitis B virus to form chronic hepatitis and cirrhosis, will eventually lead to liver cancer.
Latent infection refers to the virus lurking in the body after the primary infection, causing an acute attack indirectly. The representative here is the varicella-zoster virus infection .
Lentiviral infection means that after a dominant or stealth infection, the incubation period is quite long. Once the onset occurs, it will develop subacutely and progressively until death. Some people will classify HIV as a lentivirus infection.
The factors that affect the persistent infection of the virus are mainly viral factors and host factors.
Viral factors: The virus forms a chronic infection, immune escape occurs, the virus is latent and hidden. Some viruses form immune tolerance, such as hepatitis B and HIV.
Host factors: For example, specific T cell immune function is low, B cells cannot induce antibody production, and immune tolerance can form chronic infections. Up to now, there is no evidence of chronic infection in the new coronavirus infection.
The human anti-virus depends on various immunity, including specific immunity and non-specific immunity. Cytokines such as skin mucosal barrier and interferon are non-specific immunity. Specific immunity includes T cell mediated and B cell mediated immunity.  Human immunity is very important in immunity against viral infections After virus infection, specific antibodies can be produced, including IgA, IgM and IgG. So far, there is no reagent for IgA after infection with new coronavirus. IgM appears early and has a short duration, and is generally a sign of recent infection. IgG comes after IgM appears, appears later than IgM, lasts longer, and is a sign of previous infection. The characteristics of antibodies produced by different diseases are different. For example, after the SARS epidemic in 2003, we tested ourThe staff of the entire hospital, compared with some patients, found no patients with hidden infections. Dengue fever infection has a proportion of recessive infection. After this antibody is produced, some neutralizing antibodies have a protective effect.
Human immunity is very important in immunity against viral infections After virus infection, specific antibodies can be produced, including IgA, IgM and IgG. So far, there is no reagent for IgA after infection with new coronavirus. IgM appears early and has a short duration, and is generally a sign of recent infection. IgG comes after IgM appears, appears later than IgM, lasts longer, and is a sign of previous infection. The characteristics of antibodies produced by different diseases are different. For example, after the SARS epidemic in 2003, we tested ourThe staff of the entire hospital, compared with some patients, found no patients with hidden infections. Dengue fever infection has a proportion of recessive infection. After this antibody is produced, some neutralizing antibodies have a protective effect.
Human immunity is very important in immunity against viral infections After virus infection, specific antibodies can be produced, including IgA, IgM and IgG. So far, there is no reagent for IgA after infection with new coronavirus. IgM appears early and has a short duration, and is generally a sign of recent infection. IgG comes after IgM appears, appears later than IgM, lasts longer, and is a sign of previous infection. The characteristics of antibodies produced by different diseases are different. For example, after the SARS epidemic in 2003, we tested ourThe staff of the entire hospital, compared with some patients, found no patients with hidden infections. Dengue fever infection has a proportion of recessive infection. After this antibody is produced, some neutralizing antibodies have a protective effect.
Recently, there are reports that New Coronavirus and SARS have a certain differential immunity, and they have some epitopes in common, that is, multiple tables prepared in the future Coronavirus vaccines may prevent different coronavirus infections at the same time.
Antibody production, I just said that it has its rules. Here I take hepatitis B as an example. After viral infection, surface antigens appear first. If it is an acute infection, IgM appears one after another, and finally three antibodies appear in succession, core antibody, surface antibody, and e antibody. The vaccine only produces surface antibodies.
02 New Crown Virus Infection Disease Spectrum and Critical Warning
02 New Crown Virus Infection Disease Spectrum and Critical Warning
We understand the characteristics, outcomes and outcomes of viral infections, and we will come back to understand The clinical manifestations of new coronary pneumonia, as well as changes in some key indicators of the laboratory. We are concerned about the decrease in lymphocytes, the increase in C-reactive protein, and the increase in D-dimer, which is more pronounced in severe and critically ill patients. According to the characteristics of patients, it is divided into light, ordinary, heavy and critical. The guide is very clear, I will not repeat them here. 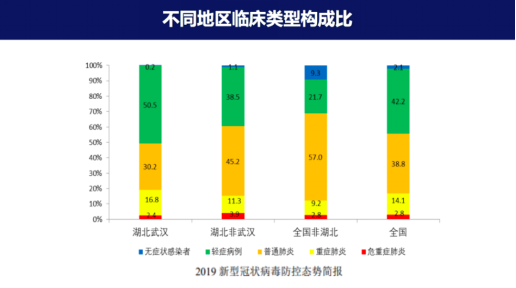 clinical types of different regions and different stages of infection The composition ratio is different. In the composition ratio of Wuhan, the proportion of critical illness and death is higher than that of non-Wuhan. Now the input patients are mainly found by rapid screening, so the proportion of mild and asymptomatic patients is higher, and the proportion of severe and dead patients will be very low. From the database of Guangdong Province, there are very few deaths.
clinical types of different regions and different stages of infection The composition ratio is different. In the composition ratio of Wuhan, the proportion of critical illness and death is higher than that of non-Wuhan. Now the input patients are mainly found by rapid screening, so the proportion of mild and asymptomatic patients is higher, and the proportion of severe and dead patients will be very low. From the database of Guangdong Province, there are very few deaths.  Age is a very important compound factor. Older people have a high proportion of critically ill patients, and the proportions of different genders are similar.
Age is a very important compound factor. Older people have a high proportion of critically ill patients, and the proportions of different genders are similar.
clinical types of different regions and different stages of infection The composition ratio is different. In the composition ratio of Wuhan, the proportion of critical illness and death is higher than that of non-Wuhan. Now the input patients are mainly found by rapid screening, so the proportion of mild and asymptomatic patients is higher, and the proportion of severe and dead patients will be very low. From the database of Guangdong Province, there are very few deaths. Age is a very important compound factor. Older people have a high proportion of critically ill patients, and the proportions of different genders are similar.
The first six editions of the guidelines did not say which patients will have indicators of increased early warning. Some indicators are listed in the seventh edition,Adult lymphocytes decline, with increased interleukin 6, C-reactive protein, and increased lactic acid, and lung lesions progress rapidly. These indicators indicate the possibility of aggravation.
We want to develop a severe risk early warning model and analyze which indicators may cause aggravation of patients, especially in high-endemic areas. Focusing on management and intervening may avoid serious consequences.
We have structurally analyzed 33 hospitals in Guangdong Province with light and moderate patients, a total of 1138 cases. We used 818 patients as the modeling team, and 320 mild patients screened by Wuhan Hankou Hospital and Honghu Hospital of Hubei Province as the verification group. All patients judge the severity of the disease according to the national standard plan.
We analyzed all patients, including clinical features and data of aggravated and non-aggravated conditions. It can be clearly seen that there is no difference between men and women. After multi-factor analysis, the age, the history of chronic diseases (diabetes, hypertension, respiratory system diseases), the ratio of white blood cells and lymphocytes, whether the C-reactive protein is greater than 25, and D- These indicators of dimer. Then we divided the patients into a low-risk group, a medium-risk group, and a high-risk group. It can be seen that almost 40% of the patients in the high-risk group will change to aggravated within 14 days of hospitalization. 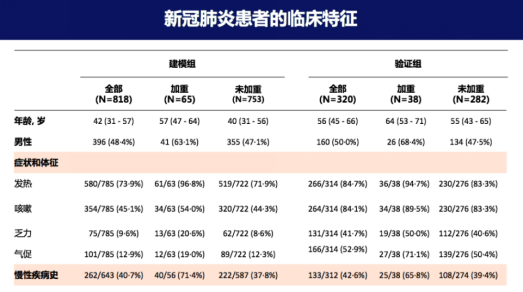 03 New Crown Virus Infection Management: Hubei Honghu model
03 New Crown Virus Infection Management: Hubei Honghu model
03 New Crown Virus Infection Management: Hubei Honghu model
We further use Honghu ’s verification group to see the same trend, and we can see that the overall aggravation ratio of Honghu is lower. We refer to the data analyzed in the early stage of Wuhan and Guangdong in the first stage. After arriving in Honghu, we will manage the patients in different levels and integrate all the medical institutions in Honghu into integrated management. The patients are divided into critically ill areas, critical early warning areas, mild wards, and discharge. In the observation area, high-risk patients are managed according to some indicators. The patients with mild diagnosis are mainly in the temporary board room hospital. The suspected patients with mild disease are also here. The discharged patients are placed in private hospitals and Chinese medicine hospitals for follow-up after discharge.  04 asymptomatic virus infection
04 asymptomatic virus infection
04 asymptomatic virus infection
As the overall domestic epidemic prevention and control situation improves, asymptomatic infection has become a hot spot. The country has specifically issued management guidelines for asymptomatic infections of new coronavirus infection pneumonia, especially in the management guidelines reiterated that asymptomatic infections are contagious and have the risk of transmission. Strengthen the monitoring and detection of asymptomatic infections, and treat asymptomatic The infection was included in the data reported in the epidemic, and the asymptomatic patients were closely observed for 14 days. You can see the recent imported cases including Guangdong, Guangzhou ’s foreign population, especially the African population, about the infection. I can tell you responsibly that there are many people on the Internet that the data on the infection of 1,000 people there is untrue. . As of April 9, I counted 1,097 patients with asymptomatic infections in 31 provinces and cities under medical observation. Of these, 349 were imported from abroad, and the number of close contacts of asymptomatic infections totaled more than 710,000.
Asymptomatic infection or subclinical infection, no clinical symptoms, and chest radiographs are also normal, mainly detected by nucleic acid means. At present, everyone is discussing whether the joint screening of nucleic acid and antibody can further help us quickly identify the type of asymptomatic infection. For example, if an asymptomatic infected person or close contact person has already produced IgG antibodies and no nucleic acid, can isolation be cancelled? This can reduce the cost of medical observation. 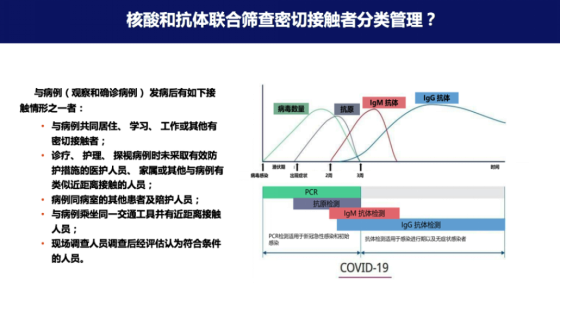 There is a set of data, which we carried out in Hubei Statistics. We used nucleic acid and two antibody kits to detect the nucleic acid and antibody of 747 close contacts. We can see that in the overall proportion of patients with positive nucleic acid, 28 people were positive for nucleic acid, which is more than 3% overall. I also asked the CDC in Guangzhou. They had almost 4,000 close contacts to screen for nucleic acids, and almost 2% of them were positive. In this way, you can see that the levels of antibodies in the population of nucleic acid positive and negative close contact with the population, you can see that the levels of antibodies in the nucleic acid positive and negative close contacts are similar. The proportion of antibodies produced by different ages is similar, there is no difference between men and women.
There is a set of data, which we carried out in Hubei Statistics. We used nucleic acid and two antibody kits to detect the nucleic acid and antibody of 747 close contacts. We can see that in the overall proportion of patients with positive nucleic acid, 28 people were positive for nucleic acid, which is more than 3% overall. I also asked the CDC in Guangzhou. They had almost 4,000 close contacts to screen for nucleic acids, and almost 2% of them were positive. In this way, you can see that the levels of antibodies in the population of nucleic acid positive and negative close contact with the population, you can see that the levels of antibodies in the nucleic acid positive and negative close contacts are similar. The proportion of antibodies produced by different ages is similar, there is no difference between men and women.
There is a set of data, which we carried out in Hubei Statistics. We used nucleic acid and two antibody kits to detect the nucleic acid and antibody of 747 close contacts. We can see that in the overall proportion of patients with positive nucleic acid, 28 people were positive for nucleic acid, which is more than 3% overall. I also asked the CDC in Guangzhou. They had almost 4,000 close contacts to screen for nucleic acids, and almost 2% of them were positive. In this way, you can see that the levels of antibodies in the population of nucleic acid positive and negative close contact with the population, you can see that the levels of antibodies in the nucleic acid positive and negative close contacts are similar. The proportion of antibodies produced by different ages is similar, there is no difference between men and women.
Among the people in close contact, 3.7% are nucleic acid positive, and antibody positive account for 11%. Obviously, some people may not find the virus in the swallowing swabs and only detect antibodies, and this group has a large proportion of people in close contact. Now China has approved many antibody detection kits, including colloidal gold and chemiluminescence kits, and may need to conduct large-scale antibody screening to evaluate what kind of prevention and control strategies are adopted. And whether we can use nucleic acid in customsJoint inspection with antibodies to assess the patient’s infection and immune status, further classification for medical management. These are all issues that need to be discussed later.  Let ’s go back and see how to depict a group The full picture of the outcome of the new coronavirus infection. We already know exactly what proportion of patients die. The reports of different countries are different. The United States and Italy are relatively high, with a high rate of 10%. Severe and critical illnesses account for about 15%, and mild and common types account for 80%. We don’t know what proportion of hidden infections or subclinical or asymptomatic infections in different populations. I just show you that in specific Honghu areas, 11% of the people in close contact have developed antibodies. How much data is needed in other regions to further understand. Whether it is an “inverted triangle” or a “positive triangle” is still unknown. This time everyone’s concern about the concept of group immunity has caused a lot of controversy. If the mortality rate is very low and the critically ill patients are very low, then the concept of generating group immunity through natural infection may be relatively tenable.
Let ’s go back and see how to depict a group The full picture of the outcome of the new coronavirus infection. We already know exactly what proportion of patients die. The reports of different countries are different. The United States and Italy are relatively high, with a high rate of 10%. Severe and critical illnesses account for about 15%, and mild and common types account for 80%. We don’t know what proportion of hidden infections or subclinical or asymptomatic infections in different populations. I just show you that in specific Honghu areas, 11% of the people in close contact have developed antibodies. How much data is needed in other regions to further understand. Whether it is an “inverted triangle” or a “positive triangle” is still unknown. This time everyone’s concern about the concept of group immunity has caused a lot of controversy. If the mortality rate is very low and the critically ill patients are very low, then the concept of generating group immunity through natural infection may be relatively tenable.
Let ’s go back and see how to depict a group The full picture of the outcome of the new coronavirus infection. We already know exactly what proportion of patients die. The reports of different countries are different. The United States and Italy are relatively high, with a high rate of 10%. Severe and critical illnesses account for about 15%, and mild and common types account for 80%. We don’t know what proportion of hidden infections or subclinical or asymptomatic infections in different populations. I just show you that in specific Honghu areas, 11% of the people in close contact have developed antibodies. How much data is needed in other regions to further understand. Whether it is an “inverted triangle” or a “positive triangle” is still unknown. This time everyone’s concern about the concept of group immunity has caused a lot of controversy. If the mortality rate is very low and the critically ill patients are very low, then the concept of generating group immunity through natural infection may be relatively tenable.
Finally, let me summarize. Today, through some data, I shared with you why the new coronavirus infection has different outcomes and which parts of patients may change from mild and common to severe or aggravated and asymptomatic infections. Here I also particularly thank Professor Li Jie for the guidance he gave me. He provided a slide about the outcome of viral infection. Thanks also to all the colleagues who participated in the work, including Wuhan and Guangdong Medical Team, thank you very much!