The antimalarial drugs chloroquine and hydroxychloroquine have been recommended by the US President Trump as a “coronal drug” for new coronavirus pneumonia, but several recently published academic studies have questioned the effect of these drugs on the new crown.
Recently, the JAMA Cardiology of the Journal of the American Medical Association (JAMA) published a report from Harvard University Beth Israel Deaconess Medical Center BIDMC ”) research results. Researchers evaluated 90 patients with new coronary pneumonia who were treated at the medical center and found that the use of hydroxychloroquine increased the risk of electrocardiographic changes and arrhythmia in patients with new coronary pneumonia. The combination of hydroxychloroquine and azithromycin was better than hydroxychloroquine alone. The resulting rhythm changes are greater.
Both hydroxychloroquine and azithromycin may cause abnormal heart rhythm, such as prolonged QT interval, which is manifested by the longer interval between specific peaks on the electrocardiogram, which may lead to arrhythmia, Increases the likelihood of cardiac arrest, stroke, or death.
Previously, on April 24, a paper published in Nature-Medical showed that patients with new coronary pneumonia treated with hydroxychloroquine and azithromycin developed ECG abnormalities. The BIDMC study published in the Journal of the American Medical Association is intended to explore the risk and extent of QT interval prolongation in patients with new coronary pneumonia using hydroxychloroquine alone or in combination with hydroxychloroquine and azithromycin.
In this retrospective study, the researchers analyzed 90 patients admitted between March 1 and April 7, 2020, all of whom accepted Hydroxychloroquine treatment, of which 53 (59%) also received azithromycin treatment. Of the 90 patients, 44 (48.9%) were women, and the common underlying diseases were hypertension (48 cases, 53.3%) and diabetes (26 cases, 28.9%), 30 severe patients (33%), mechanical ventilation 23 patients (26%).

Clinical features of 90 patients with new coronary pneumonia
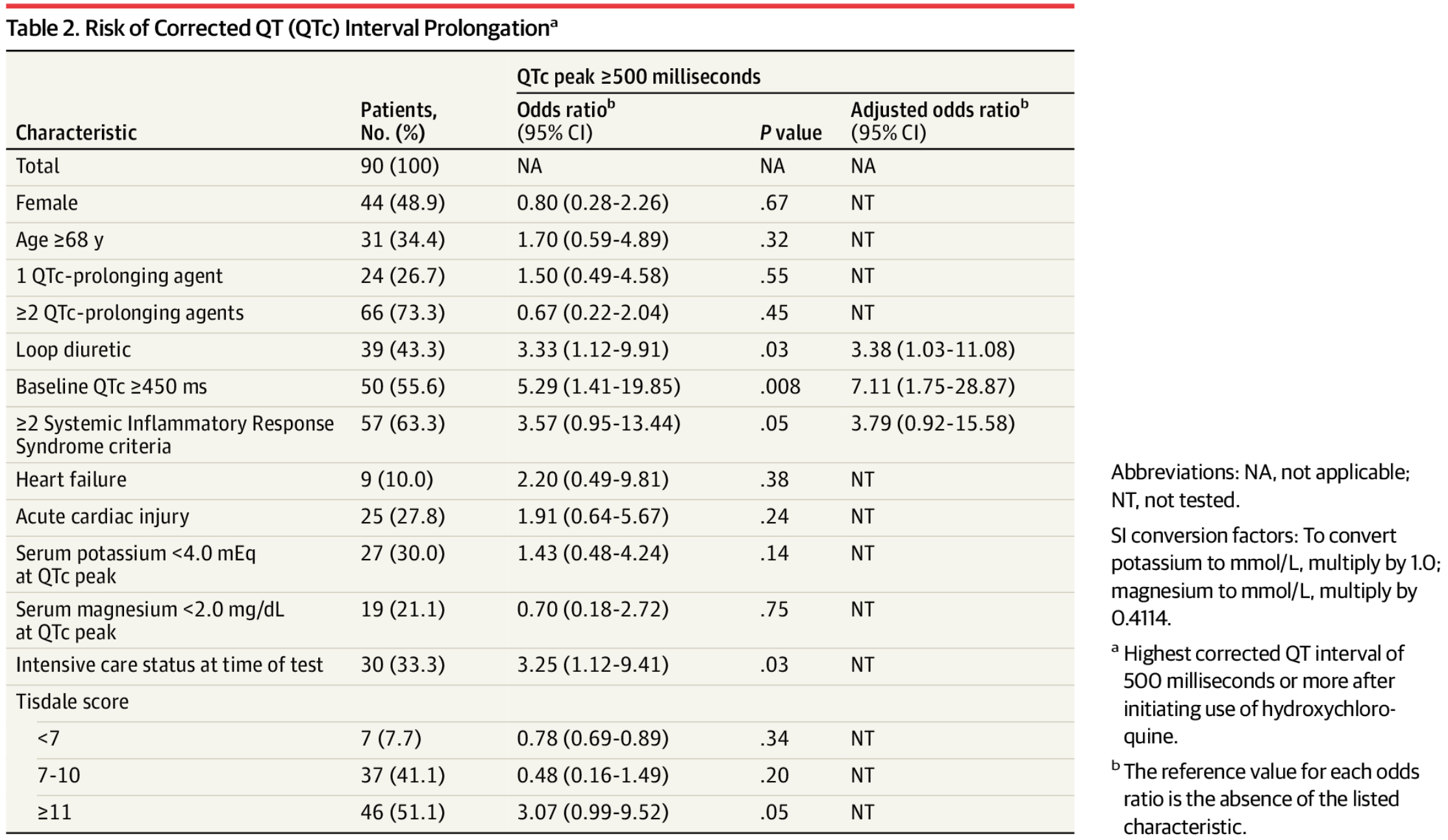 Patients are at risk of prolonged QT interval
Patients are at risk of prolonged QT interval
Clinical features of 90 patients with new coronary pneumonia
Patients are at risk of prolonged QT interval
The median baseline QT interval for these patients is 455 (430-474) milliseconds. During the 4-week observation period, 21 (23%) patients experienced significant QT interval prolongation or QT interval change (ΔQTc) greater than or equal to 60 ms.
Researchers found that compared with patients taking hydroxychloroquine alone, the combination of hydroxychloroquine and azithromycin showed a greater change in the median QT interval, two The change values are 5.5 milliseconds and 23 milliseconds, respectively.

The difference in QT interval between individuals after using hydroxychloroquine (A) or hydroxychloroquine and azithromycin (B).
The difference in QT interval between individuals after using hydroxychloroquine (A) or hydroxychloroquine and azithromycin (B).
Of the 37 new crown patients receiving hydroxychloroquine monotherapy, 7 (19%) experienced a QT interval of 500 ms or longer, 3 Cases (3%) experienced a QT interval change of 60 ms or longer. Of the 53 patients who received azithromycin and hydroxychloroquine, 11 (21%) had a QT interval of 500 ms or longer, and 7 (13%) had a QT interval of 60 ms or longer.
In addition, the researchers observed that 10 (11%) patients discontinued hydroxychloroquine before the fifth day of treatment due to prolonged QT interval. Adverse drug events that may be related to hydroxychloroquine include intractable nausea remission after discontinuation. New ventricular premature beats and right bundle branch block also appeared in the patients. A patient using hydroxychloroquine and azithromycin discontinued due to prolonged QT interval (499 milliseconds). He developed torsades de pointes ventricular tachycardia 3 days after drug withdrawal, and then developed other ventricular arrhythmias.
Twisted-point torsional ventricular tachycardia is a potentially fatal tachycardia. Christina F. Yen, co-first author of this study, said that to the best of their knowledge, after peer review In the New Coronary Pneumonia thesis, there have been no reports of acute torsion ventricular tachycardia due to the combination of hydroxychloroquine and azithromycin.
BIDMC infectious disease expert, Howard S. Gold, assistant professor of medicine at Harvard Medical School, pointed out that if you consider the use of hydroxychloroquine, especially when combined with azithromycin, clinicians should carefully weigh the risks and benefits, and closely monitor the QT interval, especially considering the underlying disease and other patients. Medication. “According to our current knowledge, hydroxychloroquine treatment of new coronary pneumonia should be limited to clinical trials. “